The Osteopathic Airway — Structure, Function, and the Whole Patient

There is a question I get asked occasionally by patients who have researched their options before coming to see me: what does DO mean, and does it change how you practice? The answer to the second part of that question is yes — and in ways that matter more for chronic airway disease than for almost any other condition I treat.
Osteopathic medicine begins with a foundational principle that the body functions as one integrated unit. Structure and function are inseparable. The physician’s role is not simply to treat the disease but to understand the patient — the whole patient — and identify what has disrupted the system rather than simply suppressing the symptom the system is generating. Thirty years of rhinologic practice have only deepened my conviction that this framework is exactly right for chronic airway inflammation, where the symptom is rarely the source and the source is rarely where anyone has been looking.
Clinical education written for patients and providers. Subscribe to the Airway & Sinus Wellness Review.
The Airway as One Connected System
The most important thing my DO training gave me — the thing I reach for every single day in clinical practice — is the reflex to look at the airway as a whole rather than as a collection of separate anatomical problems. I do not look at the nose, sinuses, throat, ears, or sleep as separate issues. I look at them as parts of one connected system, and I ask what is disrupting that system overall.
When a patient comes in with chronic sinusitis that has failed repeated antibiotic courses, the osteopathic question is not “what is wrong with the sinuses.” It is: what is disrupting the airway? Is it anatomy? Inflammation driven by allergy? Mucosal injury from silent laryngopharyngeal reflux? Lymphatic insufficiency that is impairing the clearance of inflammatory mediators from the sinonasal tissue? Sleep disruption that is impairing the glymphatic clearance of neurotoxic waste from the brain? All of these are airway questions, and all of them require a whole-patient framework to even ask.
A traditional surgical approach begins with the anatomy and asks what can be corrected. An osteopathic approach begins with the patient and asks what is disrupted. The surgical question is necessary — but it is not sufficient on its own for the patient whose disease keeps coming back after every intervention.
Structure Governs Function — From the Small Hole to the Whole Body
Osteopathic medicine teaches that structure and function are inseparable — that you cannot fully understand what a system is doing without understanding what it is built from, and you cannot understand the structure without asking what it is supposed to do. In the nose and sinuses, I have always held that the function of the nose follows the anatomy of the nose. This is not a metaphor. It is a clinical observation confirmed thousands of times in my practice.
My mentor Dr. Reuben Setliff taught me to think about the “small hole” — the principle that minimal, precise intervention that restores the natural sinus drainage opening produces better outcomes than aggressive mucosal resection. The small hole philosophy is osteopathic in its essence: work with the anatomy, not against it. Preserve structure because structure governs function. Remove only what is blocking the system, not everything that looks abnormal on a scan.
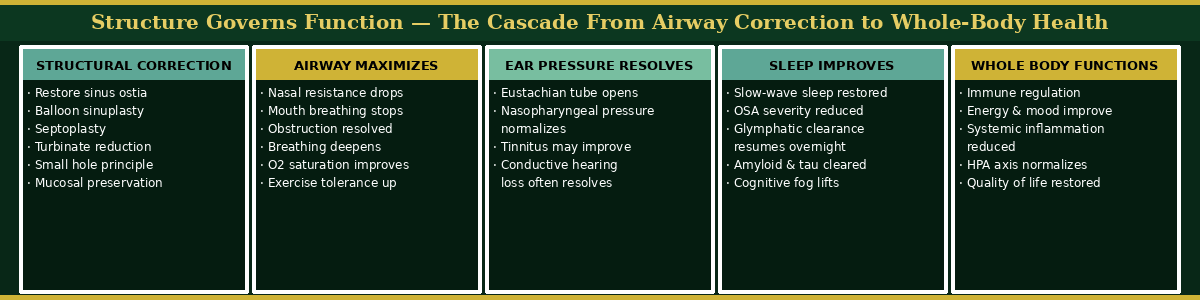
When we correct the sinus drainage openings — when we restore the natural apertures that obstruction has closed — the cascade that follows is remarkable. Nasal airway resistance drops. Breathing deepens. Ear pressure that has been present for years, driven by Eustachian tube dysfunction secondary to nasopharyngeal pressure dysregulation, often fully resolves. And when sleep improves following airway surgery, the entire body begins to function better — immune regulation normalizes, cognitive fog lifts, energy returns. This is not a surgical concept. It is an osteopathic one: structure corrected, function restored, system recalibrated.1
“The cascade below maps the whole-body consequences of structural airway correction — from restored sinus drainage through improved sleep to systemic health. Each step follows directly from the one before it, which is why treating the structure without addressing the full system leaves so many patients partially improved but never fully well.”
The Lymphatic System — An Osteopathic Tool Most ENTs Never Use
I do not perform osteopathic manipulative treatment in my office. But the lymphatic principles from my training are something I actively teach patients as part of their care, because they represent a concrete, accessible, and effective tool for managing chronic sinonasal inflammation that most ENT practices never discuss.
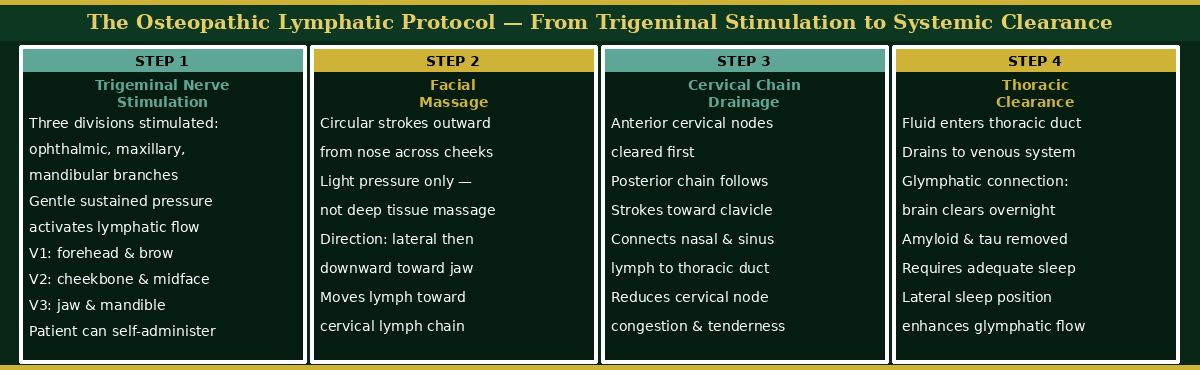
The protocol begins with stimulation of the three divisions of the trigeminal nerve — the ophthalmic branch at the forehead and brow, the maxillary branch at the cheekbone and midface, and the mandibular branch at the jaw. Gentle sustained pressure at these points activates lymphatic flow in the facial tissue. This is followed by facial massage — circular movements from the nose outward across the cheeks, then downward along the jawline toward the cervical lymph node chain. The lymph fluid is then moved down the anterior and posterior cervical chains toward the clavicle, where it enters the thoracic duct and drains into the venous system.2
The connection to the glymphatic system is direct and clinically important. The glymphatic system — the brain’s waste clearance mechanism, driven by cerebrospinal fluid flow through perivascular spaces during slow-wave sleep — drains through the meningeal lymphatic vessels into the cervical lymphatic chain.3 The same cervical chain that facial massage and lymphatic drainage techniques are targeting. This means that a patient who performs the lymphatic drainage protocol consistently, maintains adequate hydration, and protects sleep quality is not simply reducing nasal congestion. They are supporting the brain’s own overnight waste clearance system — the system implicated in the removal of amyloid beta and tau protein, the pathological proteins associated with Alzheimer’s disease.4
This is what osteopathic training gives you that a purely surgical education does not: the habit of asking what the system is connected to, and what supporting one part of it does for everything downstream.
“The protocol below illustrates the four-step osteopathic lymphatic drainage sequence — from trigeminal stimulation through facial massage and cervical clearance to thoracic drainage and glymphatic connection. Patients can perform steps one through three themselves as part of daily airway health maintenance.”
Looking Outside the Box — The Osteopathic Approach to the Patient Who Has Failed Everything
When a patient comes to me after years of treatment that has not worked — antibiotics, perhaps surgery, allergy shots, multiple specialists — the osteopathic instinct is to take a step back. Not to add another intervention to the list, but to ask what has not been asked yet. What is the root cause? What system is actually driving this, and has anyone looked at it?
In my experience, the patient who has failed everything has almost always been treated symptom by symptom, specialist by specialist, without anyone integrating the picture. The rhinologist treated the sinuses. The allergist treated the allergy. The gastroenterologist treated the reflux. But no one asked whether the silent laryngopharyngeal reflux was the upstream driver of the sinonasal inflammation that was fueling the recurring infections that the antibiotics could never resolve — because biofilm had already established itself in a mucosal environment that pepsin-driven injury had made permanently vulnerable.5
That integrative question — what is the system, what is disrupting it, and what has not been addressed — is the osteopathic contribution to rhinology. It is not a procedure. It is a clinical orientation. And for the patients who have been failed by fragmented care, it is often the most important thing I can offer them.
Dr. G’s Clinical Pearls
Pearl 1
The function of the nose follows the anatomy of the nose. Correct the structure precisely — the small hole, the natural drainage opening — and function follows. Remove more than is necessary and function suffers. My mentor Dr. Reuben Setliff taught me this, and thirty years of practice have confirmed it every time.
Pearl 2
The lymphatic drainage protocol is not a complementary therapy — it is a clinical tool. Teaching patients to stimulate the trigeminal divisions, perform facial massage, and move lymph fluid down the cervical chain gives them agency over their own inflammation between visits. It costs nothing and the evidence for lymphatic drainage in chronic sinonasal disease is real.
Pearl 3
When a patient has failed everything, the problem is almost never that the treatments were insufficient. It is that the wrong question was asked. Go back to the beginning. Ask what system is actually driving the disease. The answer is usually upstream of where everyone has been looking.
Pearl 4
The cascade from structural airway correction to improved sleep to improved glymphatic clearance to reduced cognitive symptoms is real and measurable. Treating the nose is not just treating the nose. In an osteopathic framework, it never was.
References
-
Gould J, Alexander I, Tomkin E, Brodner D. In-office, multisinus balloon dilation: 1-year outcomes from a prospective, multicenter, open-label trial. Am J Rhinol Allergy. 2014;28(2):156-163.
-
Chikly B. Silent Waves: Theory and Practice of Lymph Drainage Therapy. Scottsdale, AZ: I.H.H. Publishing; 2001.
-
Aspelund A, Antila S, Proulx ST, et al. A dural lymphatic vascular system that drains brain interstitial fluid and macromolecules. J Exp Med. 2015;212(7):991-999.
-
Xie L, Kang H, Xu Q, et al. Sleep drives metabolite clearance from the adult brain. Science. 2013;342(6156):373-377.
-
Gergits FR. The Sinus Is the Victim, Pepsin Is the Perpetrator: Posterior Sinonasal Syndrome as the Etiological Precursor to Chronic Rhinosinusitis. Preprints. 2026. doi:10.20944/preprints202603.0858.v1
Want to Understand More?
This post is part of the Journal of Airway Inflammation on the Airway & Sinus Wellness Review.
When the Airway Is the Answer — Not Just the Address
FAQ: Why Antibiotics Keep Failing Your Sinus Infection
The Final Chapter: What the Field Still Cannot See — Posterior Sinonasal Syndrome
Journal of Airway Inflammation — Clinical education from the Sinus & Allergy Wellness Center of North Scottsdale.
About the Author
Franklyn R. Gergits, DO, MBA, FAOCO is an osteopathic physician, otolaryngologist, and rhinologist with over 30 years of clinical experience. He is the founder of the Sinus & Allergy Wellness Center of North Scottsdale and performed the first balloon sinuplasty in Pennsylvania. He holds dual Entellus Centers of Excellence certifications and specializes in office-based nasal and sinus procedures under local anesthesia, including balloon sinuplasty, turbinate reduction, NEUROMARK® posterior nasal nerve ablation (Neurent Medical, FDA-cleared radiofrequency ablation system), and Eustachian tube dilation. Dr. Gergits is the originator of the Posterior Sinonasal Syndrome (PSS) hypothesis, with a preprint available at Preprints.org (DOI: 10.20944/preprints202603.0858.v1). ORCID: 0009-0000-4893-6332.
SinusAndAllergyWellnessCenter.com · 480-525-8999
This content is for educational purposes only and does not constitute medical advice. If you are experiencing sinus or airway symptoms, please consult a qualified physician for evaluation and individualized treatment recommendations.
Disclaimer:
The information provided in this article is for informational and educational purposes only and does not constitute medical advice. It is not intended to diagnose, treat, cure, or prevent any disease or medical condition. Always seek the guidance of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition or treatment.
Results may vary: Treatment outcomes and health experiences may differ based on individual medical history, condition severity, and response to care.
Emergency Notice: If you are experiencing a medical emergency, call 911 or seek immediate medical attention.
