Stress, the Autonomic Nervous System, and Airway Inflammation
One of the most underappreciated drivers of chronic airway inflammation is not an allergen, not a pathogen, and not an anatomical problem. It is stress. Not the dramatic, obvious stress of a crisis — though that matters too — but the quiet, persistent, background stress that many patients carry through every day without recognizing it as a physiological burden. The stress they have adapted to. The stress they no longer feel as stress because it has simply become the baseline.
That kind of stress does something specific and measurable to the airway. Understanding the mechanism — how stress moves from the brain through the autonomic nervous system to the nasal mucosa, the immune system, and the sleep architecture — changes how we think about airway disease and what it actually takes to treat it comprehensively.
Clinical education written for patients and providers. Subscribe to the Airway & Sinus Wellness Review.
What Stress Does to Homeostasis — and Why the Airway Pays the Price
Stress disrupts homeostasis — the body’s balanced, regulated state. When the stress response activates, cortisol and adrenaline shift every system in the body toward a state of heightened alertness and physical readiness. Blood pressure rises. Heart rate increases. Blood is redirected away from digestive and immune functions toward the large muscles. Breathing accelerates.
This cascade is adaptive when the threat is real and temporary. The problem is that chronic stress — the kind most adults in modern life carry — keeps the system in a state of sustained activation. The threat never resolves, so the body never fully returns to balance. Blood pressure remains elevated, increasing risk for stroke and cardiac events. Immune function is suppressed. Sleep is fragmented. And the airway — which depends on a well-regulated mucosal environment, a functional immune system, and restorative sleep — takes a measurable hit.1
What makes this particularly insidious is that many patients are not aware of how chronically stressed they are. The body adapts. The elevated baseline becomes normal. And the airway inflammation that results is attributed to allergy, or infection, or bad luck — not to the sustained sympathetic activation that has been degrading the mucosal defense system for months or years.
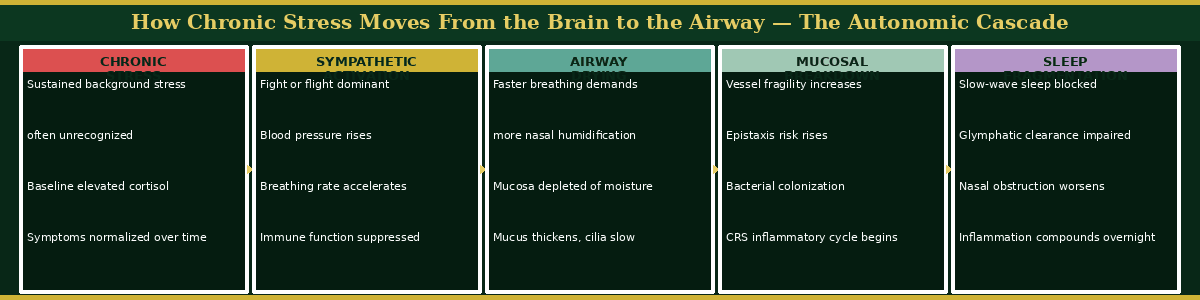
“The cascade below maps exactly how chronic stress moves from the brain through the autonomic nervous system to the airway — step by step, each stage compounding the one before it. Most patients presenting with recurrent airway inflammation are somewhere in this cascade without knowing it.”
The Autonomic Nervous System — Two States, One Airway
The autonomic nervous system governs the body’s involuntary functions through two opposing branches. The sympathetic branch — fight or flight — activates in response to perceived threat. The parasympathetic branch — rest and digest — governs recovery, repair, immune function, and restorative sleep. These two branches are not meant to be equally active at all times. They are meant to alternate — stress activates the sympathetic, the threat passes, the parasympathetic restores balance.
In chronic stress, the sympathetic branch remains dominant. The parasympathetic branch — and everything it governs — is chronically suppressed. Immune surveillance is reduced. Mucosal repair slows. Sleep quality degrades. And the nasal cavity, which reflects the autonomic state of the whole body, shows it.
When I examine a patient whose autonomic system is well balanced, the nasal mucosa is pale pink, moist, and smooth. The secretions are thin and clear. There is no thickening, no visible inflammation, no crusting. When I examine a patient under chronic sympathetic dominance, the picture is different. The mucosa is dry, irritated, and often erythematous. The secretions are thickened. The CT scan may show the mucosal changes of chronic rhinosinusitis — not because of an infection, but because the inflammatory environment created by sustained stress has degraded the mucosal defense system to the point where it can no longer maintain itself.2
How Stress Dries the Airway — The Breathing Mechanism
One of the most direct pathways from stress to airway inflammation runs through breathing rate. Stress causes us to breathe faster — often without awareness. Faster breathing means more air moving through the nasal cavity per unit of time. The nasal mucosa is responsible for humidifying every breath. When breathing rate accelerates, the humidification demand increases faster than the mucosa can meet it. The mucosal surface dries. The mucus thickens. The cilia slow. Particles and pathogens that would normally be swept away accumulate instead.3
In the desert climate of Scottsdale, where ambient humidity is already low, this mechanism is compounded. A stressed patient breathing rapidly through a dry environment is placing extraordinary demands on a nasal mucosal system that may already be depleted by inadequate hydration. The vessels in Kiesselbach’s plexus — the dense capillary network at the front of the nasal septum — become brittle. The risk of epistaxis rises. The risk of recurrent infection rises with it.
Stress, Sleep, and the Glymphatic Connection
The relationship between stress and sleep disruption is well established, but its consequences for airway inflammation are less often discussed. Chronic sympathetic activation prevents the transition into slow-wave sleep — the deep, restorative phase during which the glymphatic system clears neurotoxic waste from the brain, including amyloid beta and tau protein.4 Instead of progressing through normal sleep architecture, the stressed patient cycles through early, lighter sleep phases, waking repeatedly without completing the restorative cycles the brain and body require.
This matters for the airway directly. Nasal obstruction worsens during lighter sleep stages. The inflammatory mediators that accumulate during wakefulness — because the immune system is suppressed and clearing less efficiently — remain elevated rather than being resolved during sleep. The patient wakes more congested, more inflamed, and more fatigued than they went to bed. The cycle compounds.
Shifting From Sympathetic to Parasympathetic — Clinical Tools That Work
The goal of holistic airway therapy in the context of stress is not to eliminate stress — that is neither possible nor always desirable — but to increase parasympathetic tone deliberately and consistently, so the body spends more time in the restorative state and the airway benefits accordingly.
The 4-7-8 breathing technique is one of the most accessible and clinically effective tools for this shift. The pattern — inhale for four counts, hold for seven, exhale for eight — slows the breathing rate, extends the exhale phase, and directly activates the vagus nerve through the mechanics of slow, controlled breath. Vagal stimulation is the primary driver of parasympathetic activation.5 The extended exhale triggers the baroreflex, slowing heart rate and signaling the autonomic system to shift away from sympathetic dominance. This is not relaxation in the casual sense. It is a physiological intervention.
Humming produces a similar effect through a different mechanism. The vibration of sustained humming stimulates the vagus nerve directly through its branches in the larynx and pharynx, producing nitric oxide in the nasal sinuses as a secondary effect — a vasodilator and antimicrobial agent that benefits the sinonasal environment simultaneously.6
Meditation, gratitude practice, and prayer all share a common mechanism: they redirect cognitive attention away from the threat-scanning that sustains sympathetic activation and toward present-moment awareness or positive emotional states, both of which are associated with increased parasympathetic tone and reduced cortisol. Facial self-massage and lymphatic drainage — which we address in the companion article in this series — produce parasympathetic activation through tactile stimulation of the trigeminal nerve branches and the vagally innervated cervical structures.
For patients who cannot achieve adequate autonomic regulation through these non-pharmacological approaches — particularly those with significant anxiety disorders — I recommend an honest conversation with their primary care physician about whether pharmacological support is appropriate. There is no virtue in suffering through unmanaged anxiety when effective treatments exist. The airway pays a price for untreated anxiety that compounds over time.
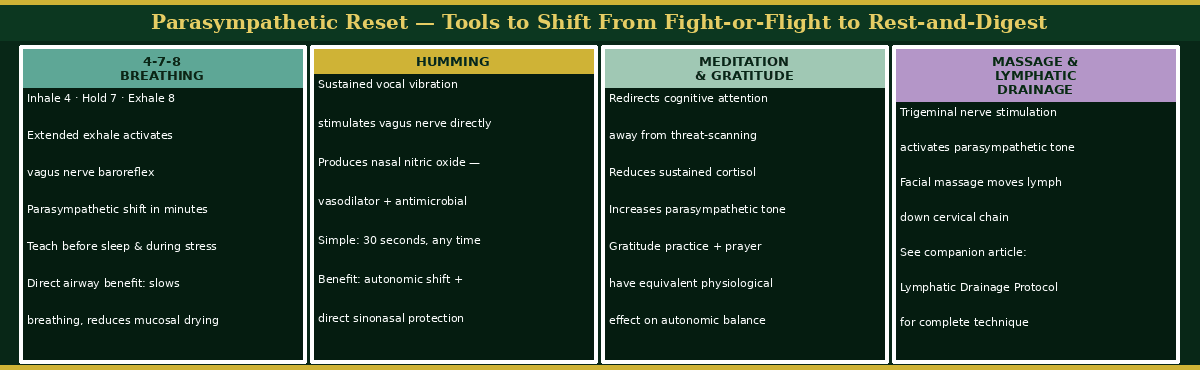
“The four tools below represent the most clinically accessible and evidence-supported methods for shifting autonomic tone from sympathetic dominance toward parasympathetic restoration. Each works through a distinct mechanism — and they are most effective when used together as a daily practice rather than reserved for moments of acute stress.”
Dr. G’s Clinical Pearls
Pearl 1
Many patients with chronic airway inflammation are chronically stressed — and do not know it. The body adapts to sustained sympathetic activation and the elevated baseline becomes invisible. When the history does not explain the inflammatory picture, ask about stress. The answer is almost always more significant than the patient initially reports.
Pearl 2
Faster breathing dries the airway. When stress accelerates breathing rate, the nasal mucosa cannot humidify air fast enough and mucosal drying follows. This mechanism is direct, measurable, and correctable — and it begins with teaching patients to slow down.
Pearl 3
The 4-7-8 breathing technique is a clinical tool, not a wellness trend. The extended exhale activates the vagus nerve and triggers the baroreflex, producing genuine parasympathetic shift within minutes. I teach it to every airway patient who presents with stress as a contributing factor — including patients with recurrent epistaxis, for whom autonomic down-regulation directly reduces bleeding risk.
Pearl 4
Humming is underutilized in clinical airway medicine. Sustained humming produces vagal stimulation and sinonasal nitric oxide simultaneously — a parasympathetic shift combined with a direct antimicrobial and vasodilatory effect in the very tissue we are trying to protect. It costs nothing and takes thirty seconds.
References
-
Segerstrom SC, Miller GE. Psychological stress and the human immune system: a meta-analytic study of 30 years of inquiry. Psychol Bull. 2004;130(4):601-630.
-
Thews O, Vaupel P. Autonomic nervous system. In: Vegetative Physiologie. Berlin: Springer; 2005.
-
Eccles R. Mechanisms of the placebo effect of sweet cough syrups. Respir Physiol Neurobiol. 2006;152(3):340-348.
-
Xie L, Kang H, Xu Q, et al. Sleep drives metabolite clearance from the adult brain. Science. 2013;342(6156):373-377.
-
Zaccaro A, Piarulli A, Laurino M, et al. How breath-control can change your life: a systematic review on psycho-physiological correlates of slow breathing. Front Hum Neurosci. 2018;12:353.
-
Weitzberg E, Lundberg JO. Humming greatly increases nasal nitric oxide. Am J Respir Crit Care Med. 2002;166(2):144-145.
Want to Understand More?
This post is part of the Journal of Airway Inflammation — Holistic Therapy for Airway Inflammation series on the Airway & Sinus Wellness Review.
The Osteopathic Airway — Structure, Function, and the Whole Patient
FAQ: Why Antibiotics Keep Failing Your Sinus Infection
The Final Chapter: What the Field Still Cannot See — Posterior Sinonasal Syndrome
Journal of Airway Inflammation — Holistic Therapy for Airway Inflammation · Airway & Sinus Wellness Review · fgergitsdo.substack.com
About the Author
Franklyn R. Gergits, DO, MBA, FAOCO is an osteopathic physician, otolaryngologist, and rhinologist with over 30 years of clinical experience. He is the founder of the Sinus & Allergy Wellness Center of North Scottsdale and performed the first balloon sinuplasty in Pennsylvania. He holds dual Entellus Centers of Excellence certifications and specializes in office-based nasal and sinus procedures under local anesthesia, including balloon sinuplasty, turbinate reduction, NEUROMARK® posterior nasal nerve ablation (Neurent Medical, FDA-cleared radiofrequency ablation system), and Eustachian tube dilation. Dr. Gergits is the originator of the Posterior Sinonasal Syndrome (PSS) hypothesis, with a preprint available at Preprints.org (DOI: 10.20944/preprints202603.0858.v1). ORCID: 0009-0000-4893-6332.
SinusAndAllergyWellnessCenter.com · 480-525-8999
This content is for educational purposes only and does not constitute medical advice. If you are experiencing chronic stress, anxiety, or airway symptoms, please consult a qualified physician for evaluation and individualized treatment recommendations.
Disclaimer:
The information provided in this article is for informational and educational purposes only and does not constitute medical advice. It is not intended to diagnose, treat, cure, or prevent any disease or medical condition. Always seek the guidance of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition or treatment.
Results may vary: Treatment outcomes and health experiences may differ based on individual medical history, condition severity, and response to care.
Emergency Notice: If you are experiencing a medical emergency, call 911 or seek immediate medical attention.
