The SAWC Sinus Burden Score — A New Framework for Measuring, Phenotyping, and Treating Upper Airway Disease
By Franklyn R. Gergits, DO, MBA, FAOCO · Sinus & Allergy Wellness Center of North Scottsdale · Scottsdale, Arizona
Estimated reading time: 12 minutes · Approximately 2,800 words · 15 references
No validated composite score currently exists that integrates sinonasal symptoms, Eustachian tube dysfunction, nasal obstruction, sleep disruption, cognitive impairment, psychological burden, and lower airway comorbidity into a single instrument — with the additional ability to classify patients into actionable clinical phenotypes and map them to a stepwise treatment pathway. The SAWC Sinus Burden Score is a proposed framework to fill that gap.
Every day in our practice, I encounter patients who have been told their sinus disease is mild — because their SNOT-22 score was acceptable. Their ear fullness was attributed to something else. Their brain fog was dismissed as stress. Their chronic cough was referred to a pulmonologist who could not find a cause. Their sleep was broken but nobody connected it to their nose. And their numbers, on the individual instruments their previous physicians used, were never quite bad enough to justify the intervention they needed.
The instruments were not wrong. They were incomplete.
What these patients needed was not a better score on one questionnaire. They needed a framework that could see all of their burdens at once — and tell both the patient and the clinician what was actually driving the full picture. That is what the SAWC Sinus Burden Score is designed to do.
The problem with how we currently measure sinus disease
The field of rhinology has fifteen validated patient-reported outcome measures for chronic rhinosinusitis. The SNOT-22 is the most extensively studied — a 22-item instrument with five validated subdomains (nasal, ear/facial, sleep, function, and emotion) and a well-established minimally clinically important difference of 8.9 to 12 points. It is an excellent instrument for what it measures. But it was not designed to capture Eustachian tube dysfunction, nasal airway obstruction as a distinct construct, obstructive sleep apnea risk, laryngopharyngeal reflux, brain fog, or the burden of acute exacerbations over the previous 12 months. Those domains require separate instruments — the ETDQ-7, the NOSE scale, the STOP-BANG, the Reflux Symptom Index — each with its own scoring range, its own psychometric properties, and its own clinical threshold. A complex airway patient completing all of them simultaneously faces more than 60 items across four different scoring systems that produce four different numbers that no one has ever synthesized into a single actionable picture.
The closest published precedent is the DAMADECO score, published in 2025 — a composite instrument combining asthma and chronic rhinosinusitis with nasal polyps into a single score ranging from negative 8 to positive 8. It was piloted in 21 patients. It does not include ETD, sleep, cognition, psychological burden, or the acute exacerbation dimension. It does not classify patients into phenotypes. And it does not map those phenotypes to a treatment pathway.
A 2015 systematic review of CRS patient-reported outcome measures explicitly identified the need for future instruments that incorporate “clinical domains that assess common comorbid diseases along with patient values and preferences.” That call has gone unanswered for a decade.
The SAWC Sinus Burden Score is our answer.
The good day / bad day / average day problem — and why it matters
One of the most clinically important questions we ask every new patient at SAWC is deceptively simple: is today a good day, a bad day, or an average day?
That question changes everything about how we interpret what we see on the CT scan and what the patient reports on the questionnaire. If a patient is having a bad day and the imaging shows active infection — that is the acute picture. If a patient is having a good day and the CT still shows chronic changes — that is the baseline burden, and it tells us what a bad day looks like even when we are not seeing it directly. If a patient is having an average day and tells us exactly how they feel in that moment — we can begin to establish what we call their sinus burden level.
No existing instrument captures this temporal dimension. The SNOT-22 asks about the past two weeks. The ETDQ-7 asks about the past month. Neither asks the patient to anchor their responses to where today falls relative to their typical experience. The result is that two patients with identical SNOT-22 scores may have completely different disease trajectories — one completing the questionnaire on their worst day in six months, the other completing it on their best.
The SAWC Sinus Burden Score incorporates a temporal modifier — Good Day, Average Day, or Bad Day — that is applied to the patient-reported domains at the time of administration. This normalizes the snapshot to an estimated average burden, allows the score to be meaningfully compared across visits regardless of where each visit falls in the patient’s symptom cycle, and creates the foundation for tracking true disease trajectory over a full treatment plan.
The following diagram illustrates the nine-domain structure of the SAWC Sinus Burden Score — how each validated sub-instrument maps to its domain, and how the six clinical phenotype buckets emerge from the pattern of elevated domain scores.

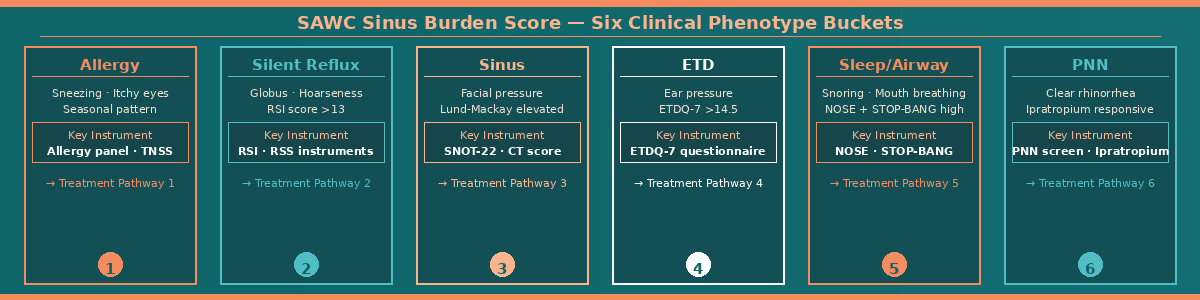
The six clinical phenotypes — and what the score reveals
The most clinically transformative feature of the SAWC Sinus Burden Score is not the composite number itself. It is what happens when the domain scores are analyzed together — the pattern of elevated scores routes the patient into one or more of six clinical phenotype buckets, each representing a distinct upstream driver of their airway disease.
The Allergy Bucket is identified when the sinonasal domain is elevated alongside positive allergy screening items — itchy nose, watery eyes, sneezing fits, seasonal pattern, and known allergen triggers. These are the patients whose sinus disease is driven by allergic inflammation narrowing already small drainage openings on a predictable seasonal schedule. Treatment starts with allergen identification and immunotherapy before any procedural intervention is considered.
The Silent Reflux Bucket is identified when the Reflux Symptom Index exceeds the established threshold of 13, and when throat clearing, globus sensation, hoarseness, and cough after meals or lying down are disproportionately elevated. These are the patients whose posterior nasal mucosal inflammation is being driven by pepsin reaching the posterior nasal cavity via laryngopharyngeal reflux — often silently, without heartburn, without any gastrointestinal complaint that would prompt a physician to ask the right questions. In my clinical framework — Posterior Sinonasal Syndrome — pepsin may be the first trigger, priming the mucosal field before any downstream sinus disease is even established.
The Sinus Bucket is identified when the sinonasal domain and acute exacerbation domain are both elevated alongside objective CT findings. These are the patients with confirmed chronic rhinosinusitis, recurrent antibiotic courses, and a Lund-Mackay score that tells the clinical story the patient has been trying to tell for years. Treatment is targeted, culture-directed, and in many cases procedural — but only after the upstream triggers have been identified and addressed.
The ETD Bucket is identified when the ETDQ-7 total exceeds 14.5 — the threshold that carries 100% sensitivity and 94.2% specificity for clinically significant Eustachian tube dysfunction. These are the patients who have been told their ears are fine because the audiogram is normal. Their ear is not fine. The tube is not opening. The posterior nasal mucosal inflammatory field that includes the Eustachian tube opening is swollen, and until that field is treated, the ear will not recover.
The Sleep and Nasal Airway Bucket is identified when the NOSE score and STOP-BANG score are both elevated — nasal obstruction driving mouth breathing, jaw displacement, posterior tongue movement, and oropharyngeal narrowing at night. These are the patients whose cardiovascular system is under chronic sympathetic stress while they sleep because their nose cannot do its job. The airway problem is not in the throat. It starts in the nose.
The Posterior Nasal Nerve Bucket is identified when constant clear rhinorrhea is disproportionately elevated, postnasal drip is the patient’s primary complaint, drainage persists regardless of whether an active infection is present, and — critically — ipratropium nasal spray has provided at least partial relief. Published data confirm that ipratropium responsiveness predicts outcomes for posterior nasal nerve ablation with meaningful accuracy. These are the patients for whom NEUROMARK® is the right answer — not more antibiotics, not more antihistamines, but direct treatment of the overactive nerve network driving the secretory hyperdrive.
Most complex patients will qualify for two or three buckets simultaneously. That overlap is itself clinically informative — it tells the clinician which upstream drivers are active, which treatment sequence is most likely to succeed, and why previous single-domain interventions have failed.
The scarred immune system — and what it means for treatment sequencing
There is a category of patient I think about more than any other — the one who comes to us after being seen by two, three, or four other ENT physicians. Discharged. Told there is nothing more to offer. Living a life of chronic high sinus burden with no pathway forward.
These patients are not difficult because their disease is fundamentally different. They are difficult because the upstream trigger was never identified, and in many cases because previous surgery removed too much. We were all trained in an era when aggressive mucosal resection was standard — strip out the diseased lining, open the sinuses wide, let it heal. What grows back into an aggressively resected sinus is not normal respiratory mucosa. It is squamous epithelium — the wrong type of tissue for a sinus cavity. It cannot perform mucociliary clearance. It may generate chronic inflammatory signals on its own. The patient who had surgery elsewhere and has never felt right since may be dealing with a mucosal lining that has been fundamentally altered.
I call this the scarred immune system — a sinonasal lining that has been chronically inflamed for so long, or structurally altered by previous surgery, that it no longer responds normally to standard treatment. These patients need a reset — a sustained period of targeted upstream treatment, autonomic rebalancing, mucosal support, and careful procedural intervention — before meaningful recovery is possible.
The SAWC Sinus Burden Score tracks this reset. By measuring the composite score at every visit — and tracking each individual domain and each individual item over time — we can see which buckets are responding and which are not. We can see whether the Silent Reflux bucket is clearing as LPR treatment takes effect. We can see whether the PNN bucket is improving after NEUROMARK®. We can see whether the Sleep bucket is normalizing as nasal obstruction is addressed. The score becomes not just a measurement tool but a treatment navigation instrument.
The following diagram shows the nine-step treatment escalation ladder mapped to each clinical phenotype bucket — from education and lifestyle optimization through autonomic rebalancing, medical therapy, and conservative in-office procedures to functional endoscopic sinus surgery for the most refractory cases.
The treatment escalation ladder — from education to surgery
The SAWC Sinus Burden Score is not a number for its own sake. Every composite score and bucket classification maps directly to a position on a nine-step treatment escalation ladder — a structured pathway that begins with the least invasive intervention and escalates only when the current step has been optimized and the score confirms it is not sufficient.
Step one is education — the patient understanding what their score means, which buckets they are in, and what is driving their disease. This is not a trivial step. A patient who understands that their constant runny nose is driven by an overactive posterior nasal nerve — not a sinus infection — is a patient who will stop requesting antibiotics and start asking the right questions about NEUROMARK®.
Step two is lifestyle optimization — hydration, saline irrigation, sleep positioning, nasal breathing retraining, and dietary modification for the reflux bucket. Published data support high-volume saline irrigation as the highest-quality evidence intervention for chronic rhinosinusitis, with a standardized mean difference of 1.42 compared to no treatment. Buteyko breathing exercises have demonstrated normalization of the ETDQ-7 score in 50% of ETD patients at 12 weeks versus 24.3% in controls in a randomized controlled trial.
Step three addresses the autonomic nervous system — the recognition that chronic sinonasal inflammation keeps the sympathetic nervous system in a state of persistent activation, and that converting the patient toward parasympathetic balance through breathing exercises, meditation, heart rate variability biofeedback, and stress reduction is not complementary medicine but mechanistically grounded treatment. A meta-analysis of 51 studies confirmed that reduced heart rate variability is consistently associated with elevated inflammatory markers.
Steps four through six encompass the full medical therapy range — from first-line nasal steroid spray and antihistamine through culture-directed MicroGenDX-guided compounded antibiotic rinses delivered directly into the sinus cavity, to biologic therapy for refractory chronic rhinosinusitis with nasal polyps. Steps seven through nine cover conservative in-office procedures — balloon sinuplasty, NEUROMARK® posterior nasal nerve ablation, Eustachian tube dilation, hybrid procedure — and finally functional endoscopic sinus surgery for the patients whose disease cannot be adequately addressed in the office setting.
The key principle: no patient should reach step seven without having completed and documented steps one through six. The SAWC Sinus Burden Score provides that documentation — a longitudinal record of what was tried, when, and what the score showed in response.
Dr. G’s Clinical Pearls
Pearl 1. A SNOT-22 score in the acceptable range does not mean the patient is doing well. It means the instrument did not capture what is actually driving their burden. Always look at the full domain picture — not the composite alone.
Pearl 2. The good day / bad day question is not small talk. It is the most important clinical anchor in the evaluation. The same CT scan means something completely different depending on where today falls in the patient’s symptom cycle.
Pearl 3. When a patient has been failed by multiple ENT physicians, the most commonly missed trigger is the resistant bacterial biofilm complex — organisms living in a sealed sinus environment, protected by biofilm, unreachable by systemic antibiotics. MicroGenDX identifies them. Culture-directed compounded rinses delivered directly into the sinus reach them.
Pearl 4. Ipratropium responsiveness is a diagnostic test, not just a treatment. A patient whose clear rhinorrhea improves with ipratropium is telling you the posterior nasal nerve is the driver. That patient is a NEUROMARK® candidate.
Pearl 5. The scarred immune system is real. A patient who had aggressive mucosal resection elsewhere and has never recovered is not treatment-resistant — they are mucosal-architecture-altered. The lining that grew back is squamous epithelium, not respiratory mucosa. The reset takes time, patience, and a fundamentally different approach than the one that created the problem.
Where this is going — the validation pathway
The SAWC Sinus Burden Score is currently in development. The concept is being actively built and refined at SAWC through clinical observation and literature review. The formal validation pathway follows the COSMIN 2.0 Reporting Guideline — the current gold standard for patient-reported outcome measure development — and includes five phases: content validity through expert panel and patient focus groups, structural validity through exploratory and confirmatory factor analysis, construct validity through convergent and divergent testing against existing instruments, test-retest reliability, and responsiveness with minimally clinically important difference estimation.
The prospective enrollment study will be conducted under independent IRB oversight with electronic data capture through REDCap, allowing individual item-level tracking over time across each treatment arm. Every domain score, every individual question response, and every bucket classification will be stored as discrete longitudinal data points — enabling the kind of granular analysis that tells us not just whether the composite score improved, but which specific symptoms responded to which specific treatments, in which sequence, for which phenotype.
The goal is not just a validated score. The goal is a clinical decision support instrument that transforms the way complex airway patients are evaluated in rhinology — giving both the patient and the clinician a comprehensive, dynamic, longitudinal picture of burden that no single existing instrument can provide.
Want to Understand More?
This post is part of the Why Sinus Treatments Fail — And What Starts Before Them series on the Airway & Sinus Wellness Review.
→ Personalized Medicine — How SAWC Builds Your Sinus Treatment Plan
→ What Is a Hybrid Sinus Procedure — and Why Might You Need One?
→ What Is NEUROMARK® — and Could It Stop Your Chronic Runny Nose?
→ Why Your Sinuses, Ears, Drainage, and Sleep Are All the Same Problem
→ Why Do Antibiotics Keep Failing My Sinus Infection?
→ What Is MicroGenDX — and Why Does It Change How We Treat Sinus Infections?
Airway & Sinus Wellness Review — Full Publication
This post is part of the Why Sinus Treatments Fail — And What Starts Before Them series.
References
-
Rudmik L, Hopkins C, Peters A, et al. Patient-reported outcome measures for adult chronic rhinosinusitis: a systematic review and quality assessment. J Allergy Clin Immunol. 2015;136(6):1532–1540.
-
Dykewicz MS, Wallace DV, Bandi S, Mahdavinia M, Sedaghat AR. Patient-reported outcome measures in rhinitis and chronic rhinosinusitis. J Allergy Clin Immunol Pract. 2024;12(3):589–601.
-
D’Amato M, Pasqualetti P, Cantone E, et al. Proposal of a new composite score (DAMADECO) to simultaneously evaluate asthma and CRSwNP severity in comorbid patients. J Clin Med. 2025;14(4):1089.
-
Cotter RA, Lee CW, Wilson K, et al. Development and psychometric validation of the Chronic Rhinosinusitis Control Test. Rhinology. 2025;63(1):12–21.
-
McCoul ED, Anand VK, Christos PJ. Validating the clinical assessment of Eustachian tube dysfunction: the Eustachian Tube Dysfunction Questionnaire (ETDQ-7). Laryngoscope. 2012;122(5):1137–1141.
-
Holm NH, Ovesen T. The usefulness of ETDQ-7 score in assessing ETD. Clin Otolaryngol. 2025;50(2):198–204.
-
Shastri K, Gao Y, Davis SJ, et al. Normative values of the Nasal Obstruction Symptom Evaluation scale. Facial Plast Surg Aesthet Med. 2022;24(3):180–185.
-
Chung F, Abdullah HR, Liao P. STOP-Bang questionnaire: a practical approach to screen for obstructive sleep apnea. Chest. 2016;149(3):631–638.
-
Gao EY, Tan BKJ, Chan KL, et al. Chronic rhinosinusitis and cognition: a systematic review and meta-analysis. Rhinology. 2025;63(2):101–112.
-
Williams DP, Koenig J, Carnevali L, et al. Heart rate variability and inflammation: a meta-analysis of human studies. Brain Behav Immun. 2019;80:219–226.
-
Lee JT, Abbas GM, Charous DD, et al. Three-year outcomes after temperature-controlled radiofrequency ablation of the posterior nasal nerve for chronic rhinitis. Am J Rhinol Allergy. 2025;39(1):22–30.
-
Maddineni S, Hwang PH, Ayoub NF, et al. Predictive value of ipratropium responsiveness on posterior nasal nerve neurectomy outcomes in chronic rhinitis. Otolaryngol Head Neck Surg. 2025;172(4):1089–1096.
-
Rudmik L, Soler ZM. Medical therapies for adult chronic sinusitis: a systematic review. JAMA. 2015;314(9):926–939.
-
Zeng H, Chen X, Xu Y, Zheng Y, Xiong H. Buteyko breathing technique for obstructive Eustachian tube dysfunction: preliminary results from a randomized controlled trial. Am J Otolaryngol. 2019;40(2):171–175.
-
Gagnier JJ, de Arruda GT, Terwee CB, Mokkink LB. COSMIN reporting guideline for studies on measurement properties of patient-reported outcome measures: version 2.0. Qual Life Res. 2025;34(1):1–18.
About the Author
Dr. Franklyn R. Gergits, DO, MBA, FAOCO is an osteopathic otolaryngologist and otolaryngic allergist with a focus in rhinology with over 30 years of clinical experience treating sinus and airway disease in Scottsdale and the greater Phoenix metropolitan area. He is the founder of the Sinus & Allergy Wellness Center of North Scottsdale and performed the first balloon sinuplasty in Pennsylvania. He holds dual Entellus Centers of Excellence certifications and specializes in comprehensive, personalized, office-based nasal and sinus care. Dr. Gergits is the originator of the Posterior Sinonasal Syndrome (PSS) hypothesis — a clinical framework identifying pepsin-mediated posterior nasal mucosal injury as an upstream driver of chronic rhinosinusitis — and the developer of the SAWC Composite Sinus Burden Score, a novel multi-domain patient-reported outcome measure currently in development. ORCID: 0009-0000-4893-6332. Preprint DOI: 10.20944/preprints202603.0858.v1.
SinusAndAllergyWellnessCenter.com · 480-525-8999
This content is for educational purposes only and does not constitute medical advice. The SAWC Sinus Burden Score is a proposed framework currently in development and has not yet been formally validated in a peer-reviewed clinical study. Please consult a qualified physician for evaluation and treatment of your specific condition.
Disclaimer:
The information provided in this article is for informational and educational purposes only and does not constitute medical advice. It is not intended to diagnose, treat, cure, or prevent any disease or medical condition. Always seek the guidance of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition or treatment.
Results may vary: Treatment outcomes and health experiences may differ based on individual medical history, condition severity, and response to care.
Emergency Notice: If you are experiencing a medical emergency, call 911 or seek immediate medical attention.
